60-year-old male, k/c/o DM, HTN, IHD (S/P CABG), CKD Stage 5D admitted with history of multiple AVF failure (Left Radiocephaic, Left Brachiocephalic, Right Radiocephaic, Right Brachiocephalic) for permanent vascular access creation. Bilateral neck and upper limb Doppler was done, suggestive of right IJV chronic occlusion (history of right double lumen dialysis catheter insertion 6 month back and kept in situ for one month) and no good site for AVF creation. So, left IJV perm-catheter insertion was planned and inserted under fluoroscopic guidance. Post procedure flow and x-ray position was checked and it was adequate.
Initial 2 dialysis sessions were uneventful. Patient went back to his hometown and started dialysis there. After 2 dialysis sessions there, flow related issues started; thus, the dialysis technician tried to flush the catheter with heparin but the flow was inadequate due to which, he inserted a guidewire to check for any obstruction or clot. But even after that the flow issue persisted following to which, the patient came back for further evaluation for catheter dysfunction.
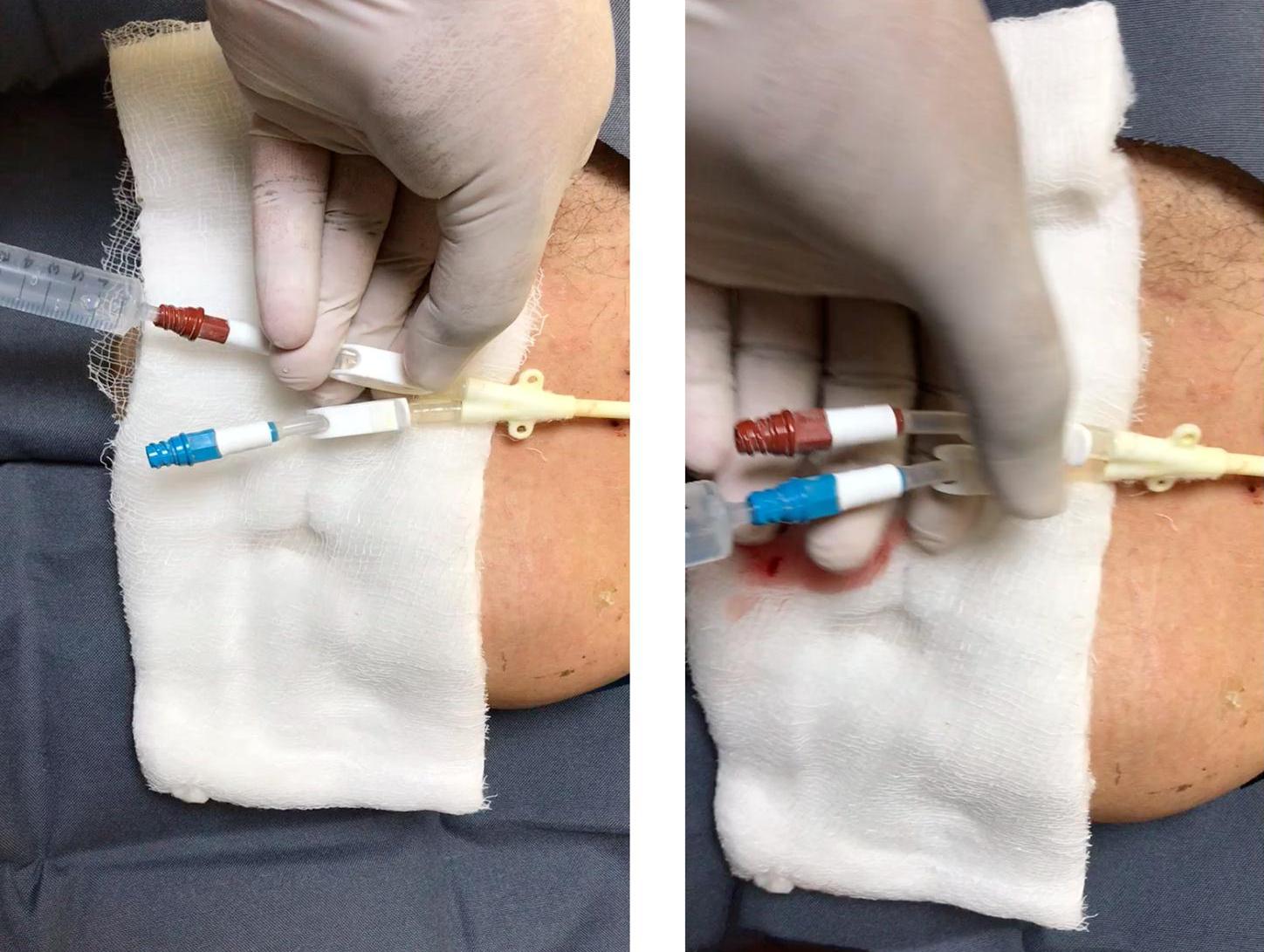
At this point, the first try was done to flush the catheter; surprisingly, the saline flushed from the red port, was oozing out from blue port and vice versa. The same can be seen in the following video.
Now the permcath was removed i/v/o significant recirculation. It can be seen that after removing the permcath, flushed saline from the blue port was oozing out from both ends. Here, the most probable reason could be the guidewire insertion which might have led to a breach in between both the lumens.
Here, after dissecting both the lumens, the rent was not evident. So, an apparent reason for this situation may be:
- Rent between the lumens that is not evident macroscopically.
- Formation of fibrin sheath (external) which led to local recirculation near the catheter tip that stopped after removing catheter
- Some other possibility which we’re not aware of.
Dialysis Catheter Dysfunction
Definition
The NKF⁄DOQI guidelines define catheter dysfunction as a failure to attain a sufficient extracorporeal blood flow of ≥300 ml/min with a pre‑pump arterial pressure lower than – 250 mmHg.
Introduction
Haemodialysis requires access to blood vessels for providing rapid extracorporeal blood flow. Temporarily cuffed, tunnelled catheters can be placed in CKD patients who require dialysis but do not have a functional permanent vascular access. Ideally, when a permanent dialysis access is required, an arteriovenous fistula is created or arteriovenous graft is placed. Once the fistula or graft is successfully functioning, the catheter can be removed.
Dialysis catheters usually have at least two lumens attached to the two ports (blue and red coloured). Generally the red port is considered the “arterial” lumen which draws blood from the body with a proximal/side opening and the blue port is considered the “venous” lumen which returns the blood from the dialysis machine to the patient with a distal opening. The direction of the flow can be occasionally reversed by dialysis technicians if it is limited to this conventional course.
Factors Associated With Dialysis Catheter Malfunction
Based on the time of occurrence, a dialysis catheter dysfunction can be classified into early or late dysfunction.
Early dysfunction usually occurs as a result of mechanical issues while late dysfunction occurs most commonly due to thrombosis.
A) Early Dysfunction
(1) Position related issues:
(a) Access site considerations
Insertion site – The right internal jugular vein is the preferred access site because the vein directly reaches the superior vena cava. Left internal jugular vein catheter needs two right angles prior to reaching the superior vena cava.
Tip position – Determining the best position for a catheter tip depends on the catheter type, insertion site and the patient’s body habitus. When patient changes from a supine to an upright or sitting position, the abdominal contents descend, the central veins lengthen, the right atrium expands, the anterior chest wall shifts downward because of gravity, and the catheter tip moves upward on an average of 2–3 cm. Larger diameter catheters move more than smaller ones and catheters inserted into the subclavian vein will retract more than those in the internal jugular vein. Catheter tip into the SVC can lead to poor flow because the tip may suck against the adjacent vascular wall during outflow. On the other hand, positioning the tip too deeply into the upper right atrium can cause arrhythmias and it may also suck against the atrial wall, which could compromise the blood flow. A catheter tip that has been positioned at the SVC-right atrial junction will rarely evoke a clinically significant arrhythmia.
Tip location should be checked by fluoroscopy or chest X -rays. Reliable radiographic landmark define the borders of the SVC which is the right tracheobronchial angle, located at a median distance of 5 cm from the SVC-atrial junction. This means that a catheter tip positioned 3 cm below the right tracheobronchial angle would always be within the SVC.
(b) Catheter malposition
Blind placement of catheter can lead to increased rate of malposition. Final position of the catheter tip depends on the course that the guidewire takes. Malposition in a small-caliber vessel can result in low blood flow and high recirculation rate that can increase the catheter dysfunction rate.
Fluoroscopy allows direct imaging of the wires and dilators to minimize the potential for injury.
(2) Kinking
Kinking is a possible when the vein insertion site is too high and an acute angle develops during tunnelling. To avoid this complication, the venotomy site in the IJV should be as close as possible to the clavicle but with a risk of pneumothorax.
(3) Catheter issues:
(a) Tip design
At present there are many designs available for catheters to increase anticoagulant lock solution contact time, to avoid stagnation of blood and vessel wall irritation. They need further evaluation as far as the catheter dysfunction rates are concerned.
(b) Coatings
Coatings are developed to improve catheter biocompatibility. Antithrombotic coatings reduce platelet adhesion, inhibit inflammatory response, and reduce thrombus formation. So in this way it may decrease the catheter dysfunction rate.
(c) Stiffness of the catheter
It is more important than the surface composition in terms of chronic endothelial injury, vessel wall abrasion and irritation. So a soft catheter would have a longer functional status.
(4) Drug precipitation
Increase in the rate of catheter malfunction occurs when there is infusion of drugs through it. Possible reasons for that are drug crystallization, drug-drug incompatibility or drug-solution incompatibility.
(5) “First use” syndrome
Gallieni and colleagues described it as a result of a “first use effect” and the contact between blood and the plastic material of the catheter, particularly inside the lumen. In these circumstances, blood flow is excellent after the insertion procedure, as well as at the beginning of the treatment; however, it shows progressive impairment during the session. The authors recommend a 24 – hour delay before using a new-tunnelled CVC, to ensure full anticoagulation and avoid this effect.
B) Late DysfunctionAs mentioned earlier, the most common reason for late catheter dysfunction is thrombosis.
(1) Thrombosis
The most important factors for thrombosis include:
- Endothelial injury during vascular access creation and during shear stress produced by turbulent blood flow
- Intraluminal stasis of blood in the interdialytic period
- Platelet activation upon attachment to the dialyzer membrane and the catheter surface
- Reduced levels of Antithrombin III and Protein-C anticoagulant activity
- Increased levels of homocysteine and fibrinogen
Insufficient anticoagulant locking solution within the catheter or leaking into the bloodstream through the side holes can promote intraluminal thrombus. The portion of the catheter distal to the side holes and towards the tip does not retain the locking solution, thus resulting in the predisposal of thrombus formation.
(2) Fibrin sheath
We have already discussed about fibrin sheath in last case report. Formation of a fibrin sheath begins at the venous insertion site and then propagates distally along the catheter. Formation often begins within 24 hours of catheter insertion and total encasement of the catheter may occur within 1 week. The sheaths are composed of a combination of fibrin, collagen, endothelial cells and thrombus (in various stages of its organization). Common presentation is outflow issues.
According to the Dialysis Outcomes and Practice Patterns Study (DOPPS), central venous stenosis occurs in up to 38% of patients with temporary central venous catheters and in 27% of patients with permanent catheters.
(3) Central vein stenosis
According to the Dialysis Outcomes and Practice Patterns Study (DOPPS), central venous stenosis occurs in up to 38% of patients with temporary central venous catheters and in 27% of patients with permanent catheters. Subclavian venous catheters have the highest rate of stenosis (40–50%) compared with internal jugular venous catheters (0–10%). The treatment options cited are Percutaneous Transluminal Angioplasty (PTA), stent placement or surgical techniques (jugular vein transposition and axillary-internal jugular vein or right atrial bypass grafting).
Article Courtesy – Dr. Jigar Shrimali
About him:
Dr. Jigar Shrimali has completed his DM (Nephrology – Gold Medalist) from I.K.D.R.C. – ITS, BJ Medical College, Ahmedabad, Gujarat. He is currently working as a consultant Nephrologist and Transplant Physician in Ahmedabad, Gujarat. He is also keen on academic programs for which he has conducted several workshops for resident doctors, physicians and dialysis technicians covering 35+ topics on Dialysis Therapies alone. He is author of TEXTBOOK OF DIALYSIS THERAPY.




What was the reason that both the subclavians were not selected for permanent catherisation ?
Left IJV is probably the last thing for permcath insertion.
Thank u very much sir for reviewing the case.
As patient was k/c/o IHD (history of CABG 6 month back) and on dual anti platelet(clopidogrel,aspirin)
so subclavian vein was not punctured i/v/o risk of bleeding.
Thanks
Thanks, Dr Jigar Shrimali , for the good review on a common problem .
Can we consider CAPD for a few months and allow these vessels to recover.
CAPD filtration could improve the LV function too.
Thank u Dr Krishnan
Relatives were explained for CAPD
But they were not willing
Also explained for femoral permcath
Fortunately at the end Right sided AVF with transposition was tried and it is working right now.
Thank you so much for the Dysfunction of catheter is is very useful information we got..
thank u!!!