Abstract
A 15-year-old female presented with uremic symptoms and stunted growth, diagnosed to have Chronic Kidney Disease (Stage V) and started on Hemodialysis. She had an episode of generalized seizures during initial dialysis sessions. The seizures were attributed to Dialysis Disequilibrium Syndrome (DDS) after invalidating the other causes and seizure activity was controlled by high osmotic agents during Hemodialysis and other conservative measures.
Case Report
A 15-year-old girl came with complaints of easy fatigability and nausea for two years which was non-associated with any other complaints. She had a history of preterm birth with a birth weight of 1.5 kg (LBWB) and was delivered by caesarean route. Milestones were achieved as per her age; she has a normal elder sibling and no other significant family history.
She had stunted growth for age; height of 141 cms and weight 25 kgs, without any bony deformities. On general examination, she had pallor and facial puffiness with blood pressure of 140/90 mm of Hg.
On investigation, she was found to have Hb- 4.9 gm/dl, Serum Creatinine- 8.9 mg/dl, Blood Urea – 262 mg/dl, Serum Potassium- 6 mEq/L, Serum Calcium- 8.5 mg/dl, Venous Blood Gas pH – 7.1, Bicarbonate levels- 6 mmol/L. Urine microscopy reported no dysmorphic RBCs, pus cells or proteinuria. Her USG Abdomen showed bilateral shrunken kidneys (RK: 5.5cms x 2.4 cms & LK: 4.8 cms x 3 cms ) with altered Cortico-Medullary Differentiation.
Here, the patient was considered for hemodialysis. For her first dialysis, F4 Dialyzer (Aeff 0.8m2) was used with co-current flow and dialyzed for two and a half hours with one Packed Cell Volume during priming of hemodialysis. During second hour of hemodialysis, she had generalized tonic clonic convulsion for which she was taken off Dialysis. The patient had second episode of generalized tonic clonic convulsion twenty minutes after termination of hemodialysis. To investigate the etiology of seizures, fundoscopy and metabolic profile was conducted which was normal [normal serum sodium (134 mEq/l), RBS (112 mg/dl), serum calcium(7.6 mg/dl) (corrected Serum Calcium-10.4 mg/dl)].Her post-dialysis blood urea level was 161 mg/dl. She had no focal neurological deficit with normal CT Brain, MRI Brain as well as a normal EEG. She was started on anti-epileptics. The patient was kept under observation when she developed third episode of generalized tonic clonic convulsion next day for which anti epileptics were escalated. During the second hemodialysis, general tonic clonic convulsion was observed again (fourth episode) despite keeping her on full doses of three anti-epileptics (Sodium Valproate, Leveracitam and Clobazam). Her blood pressure was well controlled with anti-hypertensive (Nifedipine), her post dialysis blood pressure was 120/80 mm/Hg. On subsequent dialysis, considering DDS, high osmolar agent 25% Dextrose was administered. Gladly, the convulsions subsided thereafter.

DISCUSSION
Introduction
Dialysis Disequilibrium Syndrome (DDS) is a known complication of hemodialysis especially in children particularly when they are first started on hemodialysis. Severe DDS is now rare in adults because of the standard use of the preventive measures.
Pathogenesis:
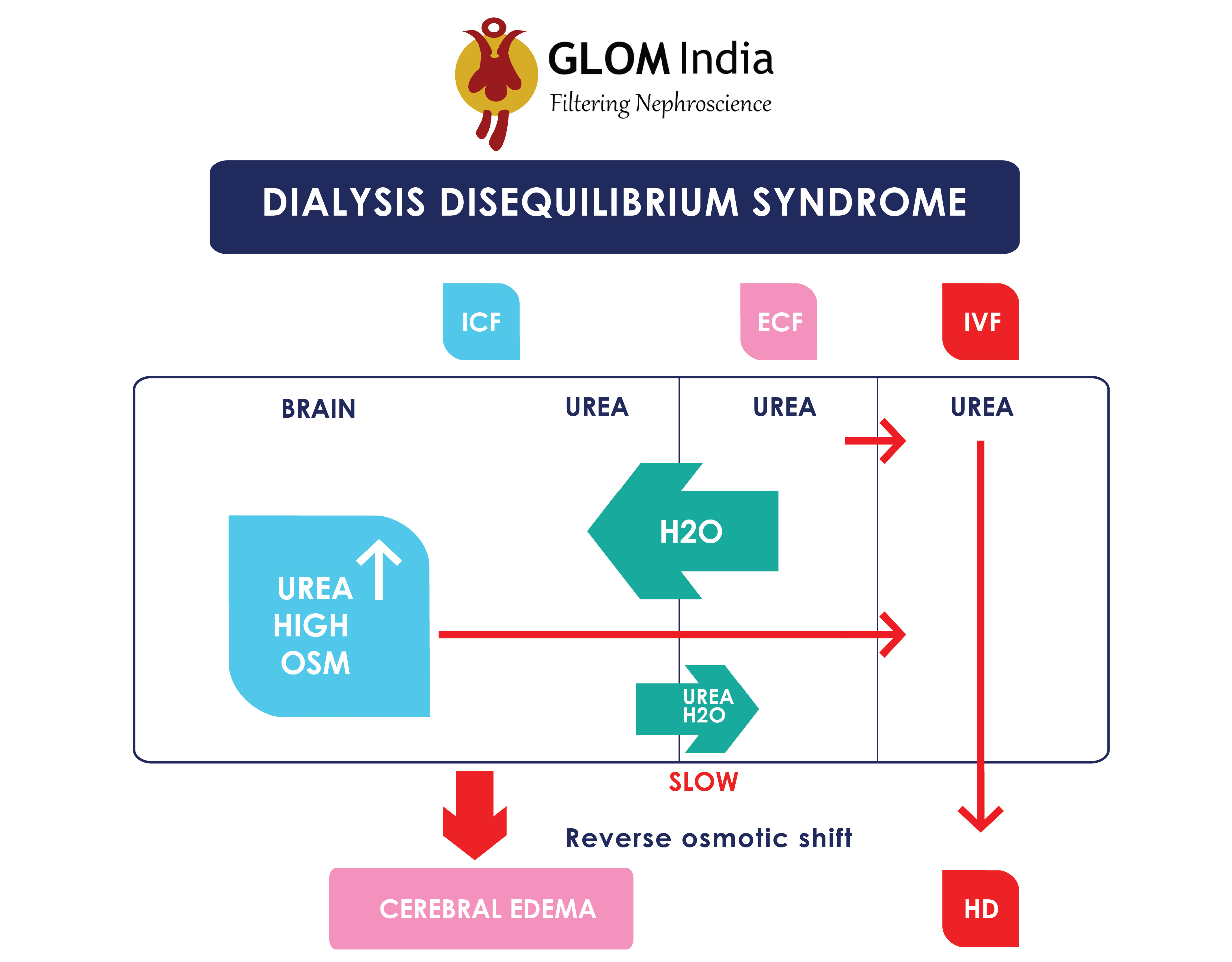
With long-standing renal failure, there is a gradual accumulation of waste products within the body, including the brain cells so when through dialysis these waste products are removed, the equilibrium in the brain cells rapidly gets disturbed which leads to cerebral oedema. Fall in cerebral intracellular pH is second theory.
Risk factors for DDS:
- First dialysis session
- Pre-dialysis blood urea concentration (>175 mg/dL)
- Chronic kidney disease (as compared with acute kidney injury)
- Severe metabolic acidosis
- Older age
- Pediatric patients
- Pre-existing neurologic disease (head trauma, stroke, seizure disorder)
- Other conditions (hyponatremia, hypocalcemia, hepatic encephalopathy, malignant hypertension)
- Any condition that increases permeability of the blood-brain barrier (such as sepsis, vasculitis, encephalitis or meningitis)
Clinical presentation
Classic DDS develops during or immediately after hemodialysis.
DDS presents with spectrum of systemic and neurologic symptoms which include:
- Nausea & vomiting
- Headache
- Restlessness
- Hypertension
- Slurred speech
- Seizure and coma (in severe cases)
Management
It is the only condition where we need to have less efficient dialysis. DDS has not been reported with continuous peritoneal dialysis and very rare with CRRT due to slow rate of solute removal.
But before we infer that the convulsions are secondary to DDS one needs to exclude its common etiologies which may be metabolic causes, structural neural damages or even hypertensive encephalopathy. It is imperative to look for hypoglycemia, hyponatremia and hypocalcemia post dialysis and strictly recommended to correct the same. In the above case, electrolyte imbalance was ruled out, sugar levels were normal, CT Brain Imaging showed no structural damage; MRI Imaging study was performed to investigate for Posterior Reversible Encephalopathy Syndrome (PRES) and Intracranial bleed and to add, EEG was also normal. Hypertensive encephalopathy was excluded as the blood pressure was controlled with Nifedipine to attain Blood pressure of 120/80 mm of Hg post dialysis, despite which episodic seizures continued. The anti-epileptics were escalated (Sodium Valproate, Leveteracetam and Clobazam).
A possibility of sudden correction of acidosis can be considered as the seat of seizures. It was noted that there was a sudden reduction in urea levels (Pre-dialysis Urea level – 262 mg/dl and post Dialysis Urea level- 161 mg/dl) which may also give rise to convulsive state. A F4 Dialyzer with co-current flow, low flow rate of 150 ml/hr with an Ultra filtrate goal of 750 ml was used to reduce the effects of sudden osmolar (Urea) shift despite which seizures were encountered. The convulsions were considered due to DDS and subsequently patient was given high osmolar agent during dialysis. No new episodes of convulsions were encountered thereafter.
The treatment of DDS depends upon the severity of symptoms:
- Patients with mild, nonspecific symptoms, such as nausea, vomiting, restlessness, and/or headache, are treated symptomatically; however, for the acutely uremic patient with such symptoms who is undergoing dialysis, the blood flow rate should be slowed, and consideration should be given to stopping the dialysis session.
- Dialysis should be stopped in the patient with seizures, coma, and/or obtundation. Patency of the airway should also be ensured. In this setting, causes of these symptoms other than severe DDS should be considered.
- Use hypertonic saline or mannitol for the treatment of DDS can be considered in refractory cases. In this case we have used intravenous D25% an after that seizures subsided.
Also, instead of treating DDS, measures to prevent DDS should be used among patients at high risk. The most important preventive measure is to limit the reduction in urea nitrogen per treatment so that there is a gradual reduction that is distributed over several days.
Slow urea removal can be achieved by the following methods:
1. Change in Hemodialysis Prescription as per below:
- Two hours of dialysis
- Relatively low blood flow rate of 150 to 250 mL/min
- Co-current flow of blood and dialsate
- Small surface area dialyzer (0.9 to 1.2 m2)
- This regimen is repeated daily for three or four days.
¯
If the patient shows no signs of DDS, the blood flow rate can be increased by 50 mL/min per treatment (up to 300 to 400 mL/min), and the duration of dialysis can be increased in 30-minute increments (up to four or more hours, as necessary for adequate solute removal).
2. Patients who also have marked fluid overload can be treated with ultrafiltration (which removes less urea per unit time), followed by a short period of hemodialysis.
3. Among patients with extremely elevated BUN concentration or neurologic symptoms, dialysis should be initiated as an inpatient.
Conclusion
Dialysis Disequilibrium Syndrome as an etiology of new onset convulsions on dialysis should be considered after exclusion of other common causes. An infusion of high Osmotic Agent during Dialysis can be used for treatment of refractory cases of Dialysis Disequilibrium Syndrome with other conservative measures.
About Dr. Vipul Gattani:
Dr. Vipul obtained DM in Nephrology from B J Medical College, Ahmedabad. Earlier he did MD in General Medicine from Maharashtra University of Health Sciences.
About Dr. Siddhi Sane:
Dr. Siddhi Sane is a third year resident, General medicine at Dr. Vasantrao Pawar Medical College, Nasik.




succinctly written.
Great site you have here.. It’s difficult to find high-quality writing
like yours nowadays. I honestly appreciate people like you!
Take care!!
Hi Dr. Vipul, Thank you very much for the great details first. You have clearly mentioned each and every Important facts.
However dialysis disequilibrium has become a uncommon complication now a days. I have not seen any of the patient with DDS with in more than 10,000 dialysis sessions yet. Although it is rare, it is well known complication. Therefore the team should have identified it earlier. Is not it?
Thank you very much
Dr Sanjaya U Jayasooriya