FEMORAL PERMCATH INSERTION: IMPORTANCE OF ANATOMICAL LANDMARK AND INTERVENTIONAL NEPHROLOGY by Dr JIGAR SHRIMALI & Dr MILAN JOLAPARA
61-year-old male, k/c/o DM, HTN, IHD (S/P CABG), CKD Stage 5D admitted with history of multiple AVF failure (Left Radiocephaic, Left Brachiocephalic, Right Radiocephaic, Right Brachiocephalic). He had a history of left sided permcath insertion in the past, which was removed due to significant recirculation. Bilateral neck and upper limb doppler was done, suggestive of a bilateral IJV total occlusion and non-availability of a good site for AVF creation. Both lower limb doppler were suggestive of right side no flow in femoral vein. So, the patient was dialysed through left sided temporary femoral dialysis catheter. Plan for right side AVF with transposition near axillary region was planned but as patient developed left sided hemiparesis, it was delayed.
Meanwhile there was leakage from temporary femoral dialysis catheter around insertion site and loss of outflow from both the catheter port. However, the inflow was adequate. A guidewire was inserted and was flushed with heparinised saline and after that the flow was rechecked but still the outflow was not achieved. As temporary femoral dialysis catheter was not functioning, a plan to insert femoral permcath was done (As it was only available accessible vessel). So patient was taken in Cath Lab and under all aseptic precautions, guidewire was inserted through temporary femoral dialysis catheter and through that 16 French sheath was inserted. Inflow and outflow were checked through the sheath and it was adequate. A dye study was also done from sheath which showed narrowing of CFV(Common Femoral Vein) and part of EIV(External Iliac Vein). After removing sheath, the femoral permcath was inserted through the same guidewire, through same puncture site.
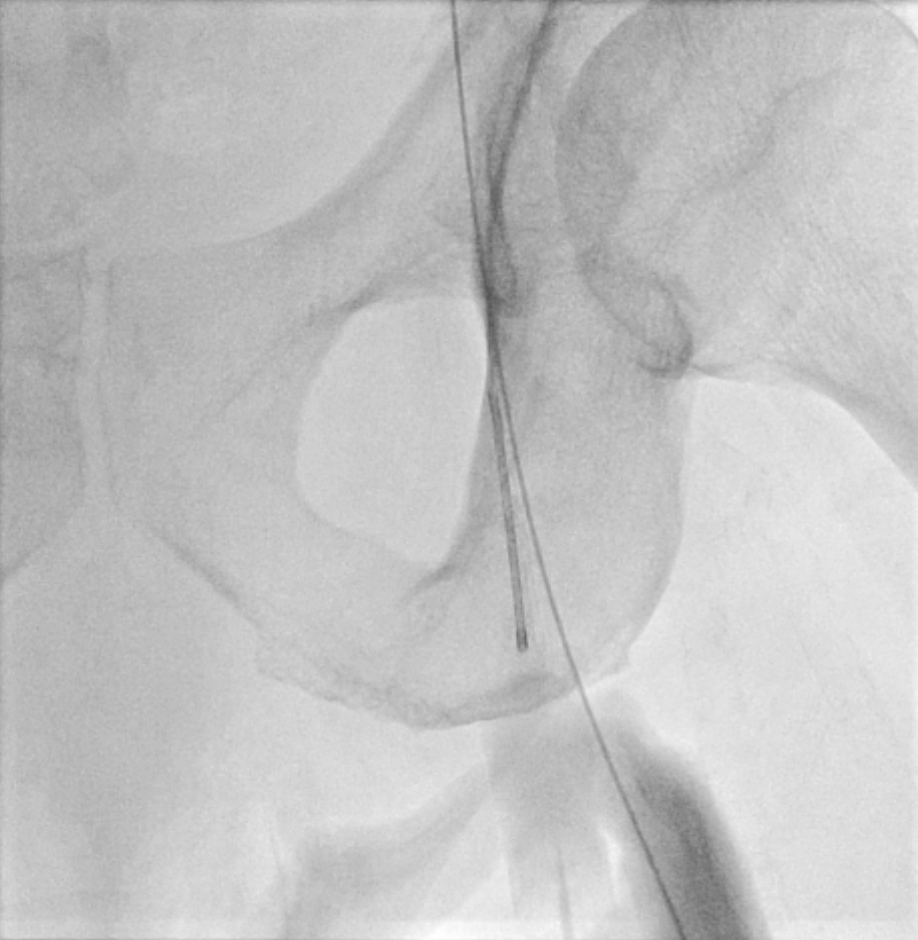
The tip of femoral permcath was in common femoral vein. The flow was checked but outflow was totally absent. A dye study was done suggesting the presence of a clot and so that permcath was removed. But as there was non-availability of any potential access site, further planning for access was required immediately. So, here issue was resettling of clot from tip of femoral permcath onwards. At this point, we planned to insert permcath through puncturing at higher site. So, it was punctured through abdomen that we never do generally but it was possible through radiological guidance in cath lab in presence of intervention radiologist.
[Note:The inguinal (groin) skin crease is usually where the inguinal ligament and common femoral artery should be punctured below it, in some obese patients there may be several skin folds below and above the presumed line of the inguinal ligament, making it at times impossible to locate the common femoral artery correctly.]
Through that sheath was inserted and vein is dilated and over it permcath was reinserted. Here the tip is in common iliac vein. Dye study was done after inserting permcath and it was showing patent pathway.
INTRODUCTION
Few points to consider:
- The common femoral vein empties into the external iliac vein, which, when joined by the internal iliac vein, forms the common iliac vein. Both the right and left common iliac veins join to form the inferior vena cava. As discussed previously the inguinal (groin) skin crease is usually where the inguinal ligament and femoral vein should be, in some obese patients there may be several skin folds below and above the presumed line of the inguinal ligament, making it at times impossible to locate the access site correctly.

- Use of radiological guidance was most important aspect of this procedure. To puncture very high blindly can lead to puncture in peritoneal cavity and that would lead to major complication. So here in a patient with non-availability of vascular access, help of intervention radiology is life-saving.
- Long term planning in view of vascular access is required. Creation of AVF in advance if dialysis is planned in near future in ESRD. The preferred type of chronic hemodialysis vascular access is arteriovenous (AV) access, rather than hemodialysis catheters. Compared with AV hemodialysis access, hemodialysis catheter use has been consistently associated with worse complication and survival rates. An AV fistula is recommended over an AV graft for hemodialysis because a mature AV fistula has the lowest morbidity and mortality, lowest need for intervention, and the best long-term patency. Venous catheters are not ideal for long-term use. With a venous catheter, a patient may develop a blood clot, an infection, or a scarred vein, causing the vein to narrow. However, if a patient needs to start hemodialysis right away, a venous catheter will work for several weeks or months until a surgeon can perform a long-term access surgery and the AV fistula or AV graft has time to mature. If fistula or graft surgery is unsuccessful, then a patient will need a long-term venous catheter access. When a patient needs a venous catheter for more than 3 weeks, the nephrologist will “tunnel” the catheter under the skin, rather than insert it directly into the vein. A tunneled catheter is more comfortable and has fewer problems.
- A longer catheter is needed when hemodialysis access is placed into the common femoral vein. Short hemodialysis catheters (<15 cm) have higher recirculation rates when the tip of the catheter is positioned in the iliac vein. A catheter length >20 cm (tip to hub) is adequate for most average-sized adults to position the tip of the catheter in the inferior vena cava, which minimizes recirculation. Very long catheters (>35 cm) should generally be avoided, as flow rate decreases with increasing catheter length, but may be needed in the rare circumstance in which an ileocaval stenosis prevented adequate dialysis with a shorter catheter.
- In the presence of occlusion of the above-mentioned veins, percutaneous translumbar insertion of the catheter into the inferior vena cava is an option of last resort that can be performed. Percutaneous insertion of the catheter into the hepatic vein can also be performed. Another approach uses open surgery to place a catheter directly into the right atrium, superior vena cava, inferior vena cava, or azygos vein. The tip of femoral hemodialysis catheters (nontunneled or tunneled) should be placed in the distal inferior vena cava to minimize recirculation. Catheters that are located in the iliac veins should be repositioned. Heparin lock has been used for decades with relative safety. However, catheter dysfunction continues to be problematic. The American Society of Interventional Nephrology position paper recommends the use of heparin lock in a concentration of 1000 units/mL. More concentrated heparin is associated with inadvertent systemic anticoagulation and clinical episodes of bleeding, particularly if the catheter lumen was overfilled. (With higher concentrations, overfilling the catheter lumen by as little as 0.1 cc could result in a heparin bolus of 500 to 1000 units). A lower heparin concentration (100 units/mL) is reasonably effective for preventing catheter thrombosis and costs less.
Article Courtesy – Dr. Jigar Shrimali and Dr. Milan Jolapara
About Authors:
Dr. Jigar Shrimali has completed his DM (Nephrology – Gold Medalist) from I.K.D.R.C. – ITS, BJ Medical College, Ahmedabad, Gujarat. He is currently working as a consultant Nephrologist and Transplant Physician in Ahmedabad, Gujarat. He is also keen on academic programs for which he has conducted several workshops for resident doctors, physicians and dialysis technicians covering 35+ topics on Dialysis Therapies alone. He is author of TEXTBOOK OF DIALYSIS THERAPY.
Dr. Milan Jolapara has completed his MD in Radiology from B J Medical College, Ahmedabad and DM in Neuroradiology from SCTIMST, Trivandrum, Kerala. He is a Consultant Interventional Neuroradiologist and Peripheral Vascular Interventionist in Ahmedabad and has his own clinic – Dev Interventional Clinic. He has an experience of more than 9 years and has completed more than 5000 interventional therapeutic procedures. Dr. Milan is affiliated with all major hospitals across Gujarat.




Very difficult situation but handled great..
Thanks Dr Raheel Ahmed
Very informative. Though I m a dialysis patient I m very much interested to know regarding dialysis in details. I follow your blogs every time. Thankyou so much.