First of all, let’s have 2 cases to discuss where catheter tip was not in ideal position, but was in anterior mediastinum.
1) INNOMINATE VEIN PERFORATION
40-year-old female with K/C/O HTN and CKD STAGE 5D, started on MHD through right IJV temporary DLC. She had poor calibre vessels for AVF creation. She developed right IJV thrombosis so left IJV permcath insertion was planned. During insertion of permcath in the left IJV, no major complications were encountered initially. Immediately before insertion of the guidewire, a continuous dark red blood return was recorded. However, there was mild resistance during guidewire insertion. On aspiration of the catheter ports, a brisk dark (venous) blood return was observed from blue port but poor flow from red port.
A check radiograph showed abnormal position of catheter tip, along the left mediastinal border (Figure 1). We further went ahead with the computed tomography angiography, which revealed a permcath puncture of the innominate vein and its malposition into anterior mediastinum (Figure 2). Catheter was removed as there was perforation of vein and close observation was done of the patient. Post catheter removal there was no complication.


| Figure 1: Chest X-ray showing straight decent of the left IJV permcath in left paramedian position. | Figure 2: Spatial reconstruction of the thoracic CT scan showing the site of permcath puncture of the innominate vein and its malposition into anterior mediastinum |
2) Persistent left superior vena cava (PLSVC)

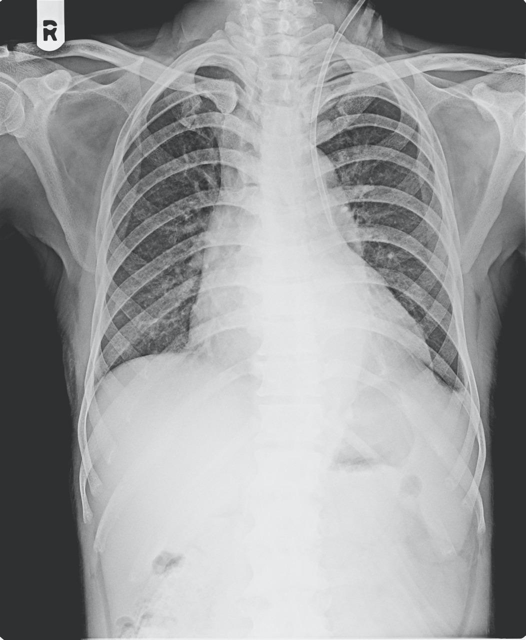
Figure 3: Chest X Ray S/O left sided temporary dialysis catheter in to persistent left SVC
52-year-old male with K/C/O HTN and CKD STAGE 5D, started on MHD through right IJV temporary DLC. He developed right IJV CRBSI, so left IJV DLC insertion was planned. During insertion of DLC in the left IJV, no resistance during guidewire insertion was noted. On aspiration of the catheter ports, a brisk dark (venous) blood return was observed. However, routine post-procedure X-ray chest showed the dialysis catheter through a left paramediastinal course from the left neck (Figure 3) and a brisk dark red blood return which was referred for blood gas analysis. The blood gas analysis performed using sample drawn from dialysis catheter was venous in nature (pH 7.3, PCO2 60 mmHg, PO2 39 mmHg, and cHCO3 21 mmol/L)
We further went ahead with the computed tomography angiography, which revealed a PLSVC. The HD sessions were easily performed with a blood flow rate of 150 ml/min. We planned to leave the catheter in place for HD, as the patient did not have any complaint and no other accessible site for HD. During the first and subsequent HD, his vitals were maintained and there was no evidence of impaired venous drainage of the left upper limb. The electrocardiogram showed no evidence of any arrhythmia or ischemia. No catheter-related complications were observed. The catheter was then used uneventfully with careful and continuous monitoring and meanwhile left BC AVF was created.
DISCUSSION
- Temporary or long term tunnelled dialysis catheters are used when AV fistula is not available for dialysis therapy. Routinely, the catheter should be inserted through a right internal jugular vein (IJV), because of the relative direct way to superior vena cava (SVC) and right atrium, and comparatively low chances of central vein stenosis. The left IJV is used only when anatomical or pathological problem in the right IJV. Alternatively, the subclavian or femoral vein can also be used. However, the catheter placement through a subclavian vein may increase the risk of stenosis and thrombosis, while femoral vein is recommended as in emergency situation.
- Cannulation of the central veins with large calibre catheters can result in complications especially on the left internal jugular vein particularly perforation or malposition considering two right angles that the catheter has to pass through during its way down to the superior vena cava. Also, such a tortuous route can cause reduced blood flow rates and greater risk of thrombosis or stenosis due to increased trauma to vessel walls.
- Haemorrhage in perforations at the level of the base of the neck can be controlled by manual compression. When deep down, balloon-assisted haemostasis and stenting or major surgery is needed depending on hemodynamic condition and severity of injury.
- The route taken by the dialysis catheter is a potential indicator of malposition and perforation during dialysis catheter placement. However, the most important indicator is no flow of blood from the ports of the catheter.
- The clinicians should be aware of this anatomic variant to prevent the complications and the unnecessary dilemma regarding the appropriate position of the catheters in place. It is important for clinician and technicians for clinical implication of catheter placements. To remove any malpositioned catheter with good blood flow is an issue considering limited access availability.
- Commonest site for catheter insertions are in thoracic region. Persistent left superior vena cava (PLSVC) is the most common congenital thoracic venous anomaly found in 0.3%–0.5% of the general population and 4% of the patients with congenital heart disease.
- Castellanos first described the left superior vena cava (LSVC) by angiocardiography. Hairston stated that the PLSVC is the most common variant of abnormal systemic venous entry into the heart.
- John Marshall gave the first embryological explanation for PLSVC in 1850. During the 8th week of gestation, an anastomosis forms between right and left superior cardinal veins leads to innominate (or brachiocephalic) vein. The cephalic portion of superior cardinal veins form the IJVs. The caudal portion of the right superior vein forms the normal right-sided superior vena cava, while the portion of the left superior cardinal vein caudal to the innominate vein normally regresses to become “ligament of marshall’. If the regression of the left superior cardinal vein fails to occur, a persistent left-sided vascular structure that empties into the coronary sinus, results into PLSVC.

- Furthermore, cardiac arrhythmias including ventricular fibrillation and atrial septal defects are associated with PLSVC. 92% of PLSVC drain into the coronary sinus and thence into the right atrium. In this circumstance, the coronary sinus is usually large due to increased blood flow through it. The rest of 8% drains into the left atrium creating right to left shunt. This variant is potentially dangerous as the cannula in PLSVC may give rise to systemic embolization of air or thrombus.
- The left and right brachiocephalic veins (or innominate veins) are major veins in the upper chest, formed by the union of each corresponding internal jugular vein and subclavian vein. This is at the level of the sternoclavicular joint.
- Placement of a catheter into anterior mediastinum can be mistaken for placement into PLSVC, carotid artery, perforated brachiocephalic vein, mediastinum or lung parenchyma.
- Real-time ultrasonography access to IJV is mandatory. Tunnelled central venous catheter should always be placed under fluoroscopy guidance. Whenever an unusual track of guidewire is noted, a venogram should be performed before placing the catheter blindly. PLSVC can be used as an optional vascular access, if no other central veins are available.
- Some nephrologists believed that PLSVC has relatively thin walls and low blood flow, making it unsuitable for long-term access to haemodialysis. Use of PLSVC as haemodialysis access was also associated with some complications, including arrhythmia, pericardial effusion, thrombus formation, and reduced blood flow to the heart. However, literature reviews of the same case show the possibility of PLSVC being used as haemodialysis access in short- and long-term haemodialysis patients, certainly with tighter monitoring.
- So, management of CVC malposition must be based on several considerations: the indication of insertion, the location of insertion, and the condition of the patient, blood flow achieved with the catheter, radiological confirmation for no perforation, arrhythmias or any congenital anomalies. If there are difficulties as in these cases, the risks and benefits of the inserted CVC must be considered. The patient in first case was with perforated brachiocephalic vein, so immediate removal of the catheter was considered to prevent worsening of the condition. Removal of the catheter in second case was not done till permanent access was created because catheter removal could have increased the issues related to non-availability of access.
-
With increasing load of CKD 5 D patients in india,difficult vascular access and associated complications are increasing!It’s time to include dedicated interventional nephrologist curriculum in our DM and DNB training program!
Dr. Siddharth H. Jain
About him:
Dr. Siddharth H. Jain is consultant Nephrologist and transplant physician, who has been extending his extending his excellent service in the field of Nephrology in Surat since 2012. After completing DM Nephrology super-speciality degree from IKDRC, Ahmedabad, he has exemplary experience in live related and cadaveric renal transplantation, as well as post-transplant care. He has got more than 15 publications in various national and international journals. He conducts CME for physicians and family physicians regularly in south Gujarat. He got recognition as ” Times Health Icon 2020″ in field of Nephrology.
Dr. Jigar Shrimali
About him:
Dr. Jigar Shrimali has completed his DM (Nephrology – Gold Medalist) from I.K.D.R.C. – ITS, BJ Medical College, Ahmedabad, Gujarat. He is currently working as a consultant Nephrologist and Transplant Physician in Renus kidney hospital, Ahmedabad, Nadiad, Gujarat. He is also keen on academic programs for which he has conducted several workshops for resident doctors, physicians and dialysis technicians covering 40+ topics on Dialysis Therapies alone. He is author of TEXTBOOK OF DIALYSIS THERAPY.


