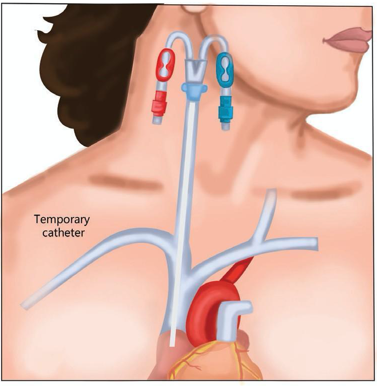
PREFERRED TEMPORARY DIALYSIS CATHETER LOCATION FOR DIALYSIS THERAPY BY DR JIGAR SHRIMALI

CVCs should preferably be inserted into the right jugular vein, as
- It carries the lowest risk of thrombosis and stenosis
- Straight course into the superior vena cava or right atrium reduces the risk of malposition and allows high blood flow
- Gives more chance to correct blind catheter tip placement considering large superficial vein
- Have easy ultrasound visualization
- Patient will be able to mobilize easier
CVC situated in the femoral vein carries an increased risk of infections and undisputed increased risk of thrombosis. But now, some newer trials show there is no major increased risk of infection with the femoral catheter. Risk for a catheter-related blood stream infection was lower for femoral lines if the body mass index (BMI) was <24.2 and for the internal jugular vein if BMI was >28(Parienti et al). Femoral lines are also preferred if emergent dialysis is needed with inexperienced operator or no ultrasound available considering avoidance of life-threatening risks such as arrhythmias, pneumothorax, hemothorax, hemomediastinum, atrial perforation. Femoral access is considered the second choice due to the higher incidence of thrombotic and infectious complications. It could be preferred in patients with bilateral occlusion of the central thoracic veins, kyphosis, severe pulmonary edema, or in people with an emergent need of vascular access. Otherwise, they are contraindicated in patients with known iliac vessel pathology, major infection risk (such as chronic diarrhea), and morbid obesity (body mass index [BMI] >35 kg/m2). Patients with ESRD right femoral catheter insertion to be avoided considering need for renal transplant.
The left IJ vein should be considered if the right internal jugular vein and femoral veins are not optimal choices. It is associated with a higher incidence of CVC dysfunction due to the two right angles that the device has to pass through during its way down to the superior vena cava. Such a tortuous route can cause reduced blood flow rates and greater risk of thrombosis or stenosis due to increased trauma to vessel walls.
The subclavian vein is the last resort with the right side being preferable considering
- Higher bleeding risk
- Higher pneumothorax risk
- Higher thrombosis risk
- “Blind” procedure that cannot be guided with ultrasound
Subclavian placement has become less frequent in clinical practice because of the notable risk of central venous stenosis that can compromise future AV access on the same side.
Dr. Jigar Shrimali
About him:
Dr. Jigar Shrimali has completed his DM (Nephrology – Gold Medalist) from I.K.D.R.C. – ITS, BJ Medical College, Ahmedabad, Gujarat. He is currently working as a consultant Nephrologist and Transplant Physician in Renus kidney hospital, Ahmedabad, Nadiad, Gujarat. He is also keen on academic programs for which he has conducted several workshops for resident doctors, physicians and dialysis technicians covering 40+ topics on Dialysis Therapies alone. He is author of TEXTBOOK OF DIALYSIS THERAPY.


